- NO OVULATION
- BLOCKED
FALLOPIAN TUBES
- SALPINGITIS
- HYDROSALPINX
& PYOSALPINX
- ENDOMETRIOSIS
- FIBROIDS & POLYPS
IN THE UTERUS
 |
Blocked fallopian tubes |
| |
|
| |
Tubes can be blocked for a number of reasons : |
| |
|
 |
Blocked from birth ( congenital tubal obstruction ) |
| |
|
|
Intentional tying or clipping ( to prevent pregnancy ) |
| |
|
|
Accidental damage following other surgery e.g. colectomy |
| |
|
|
Severe endometriosis |
| |
|
|
Inflammation ( salpingitis ) |
| |
|
| |
Of these, the last is by far the most common. |
|
Salpingitis |
| |
|
| |
Inflammation of the fallopian tubes can occur from the inside, that is, from the uterus, as is the case with sexually transmitted diseases such as gonorrhoea or chlamydia. It can also come from outside the tube by the spread of infection from another organ such as the appendix.
When this happens, the tube is often damaged by adhesions, where two damaged surfaces actually join together. Adhesions can also occur after pelvic surgery or as a result of endometriosis. Adhesions can obstruct in a number of ways - by separating the ovary and tube with new tissue or by blocking the outer end of the tube.
In many cases, microsurgery can be helpful in clearing the blockage. |
|
Hydrosalpinx & Pyosalpinx |
| |
|
|
| |
 |
A hydrosalpinx is a particular type of tubal blockage in which the tube is obstructed near its fimbrial end. The tube becomes filled with clear watery fluid. Sometimes after IVF the rise in progesterone causes the tube to relax and this fluid can be passed into the uterus, washing out the transferred embryo.
This process accounts for quite a few cases of persistent IVF failure. A pyosalpinx is an acutely inflamed blocked tube filled with pus. It sometimes subsides with antibiotics, becoming a hydrosalpinx.
|
| |
Otherwise it can rupture and form an abscess in the pelvis, much like a burst appendix, and then requires an operation to drain both it and the abscess. |
|
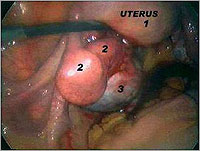
Endometriosis |
|
|
| |
|
 |
Endometriosis occurs when material similar to the lining of the uterus begins to grow outside the uterus. It is quite a common disorder, especially in women over 30 who have had no children. It may account for as many as one in 15 cases of infertility.
Severe endometriosis can distort the tubes and ovaries so much that it has a profound effect on fertility. It can also stimulate the body's resistance to foreign material, which can destroy sperm before it has a chance to reach the egg.
Recent research is suggesting that endometriosis may also produce mucus that blocks the egg from entering the fallopian tube in the first place.
|
Endometriosis is usually confirmed by laparoscopy (looking inside the abdominal cavity through a small incision in the navel) and can often be treated at the same time. It can also be treated by non-surgical methods, such as hormone control.
These treatments can help to alleviate the symptoms of endometriosis, but because they prevent ovulation they will not improve fertility while the drugs are being taken or after they are ceased. Younger women, for whom getting pregnant is not their first priority, might choose this treatment for long-term control. |
|
Fibroids and polyps in the uterus |
|
| |
|
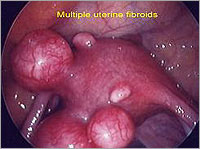 |
Fibroids are benign lumps of tissue growing in or on the myometrium (the wall of the uterus surrounding the endometrium). The closer they are to the endometrium, the more likely they are to cause symptoms such as heavy bleeding, dysmenorrhea and infertility.
Sometimes there are polyps or fibroids inside the uterine cavity called submucous fibroids. Any fibroids inside the uterine cavity must be removed prior to starting infertility treatment.
|
|

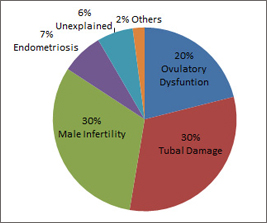
 FEMALE INFERTILITY
FEMALE INFERTILITY