- DOES THE MAN HAVE TO BE TESTED TOO ?
- IS THERE A SPERM PROBLEM ?
- IS THERE A PROBLEM WITH OVULATION ?
- IS THERE A PROBLEM WITH IMPLANTATION ?
- WHAT IS UNEXPLAINED INFERTILITY ?
 |
Does the man have to be tested too? |
|
| |
Both the partners should be evaluated simultaneously. Infertility can be due to male factors as often as female factors. Limiting the evaluation to only one member of a couple can delay or prevent doctors from understanding why a couple is not conceiving? |
| |
 History and Physical History and Physical |
The first step your doctor will take in answering the four basic questions is to get a detailed medical and a personal history from you and your partner. This includes any past medical anad surgical events, current health status including diet and lifestyle, occupational risks, history of sexual development, previous use of birth control, any past pregnancies, and current sexual practices. Concerns not shared openly between partners should be discussed privately with your doctor and will be held in confidence.
The next step is to examine both partners. The initial female examination consists of a general physical exam and a comprehensive pelvic examination . This internal examination is very helpful in providing information about the size ,shape and position of the reproductive organs . Many doctors do a routine Pap test at this time, getting a tissue sample by swabbing the cervix .This is done to rule out cervical cancer. Cervical secretions may also be cultured to detect any infection, and the woman should be tested to see if she is immune to rubella (German measles) and vaccinated if she is not.
The initial male examination also consist of a general physical, as well as a more detailed examination of the testes, penis and scrotum . During this test , the doctor seeks to detect the presence of a varicocoele, (swollen varicose veins in the scrotal sac). A culture may also be taken from the opening in the man's penis to detect the presence of infection. |
|
Is there a Sperm Problem? |
|
| |
One of the most important parts of the infertility work-up is to identify if a sperm problem exists. This may influence further testing of the woman, or indicate the need for the man to undergo treatment while the woman undergoes further testing. A semen analysis is the single most important test in the evaluation of a man's infertility. it provides valuable information related to male infertility.In addition to the semen analysis, the diagnosis of male infertility may require blood tests for FSH and LH levels, as well as for testosterone. All of these hormones plaly a role in the maturation and development of sperm in the man's reproductive system. Further physical examination for anatomical defects or abnormal conditions related to the mans reproductive organs may be necessary to help pinpoint the problem.
Tests done in the male ( see Male Infertility section ) |
|
Is there a problem with Ovulation? |
|
| |
The tests for ovulatory status are designed to determine if egg production and ovulation are occuring regularly.Usually, if a woman is menstruating regularly, she is also ovulating, but this isn't always true. A woman can be oligo-ovulatory (irregular ovulation) or anovulatory (no ovulation) and still have periods. However, her periods are generally either irregular (oligomenorrhoea) or absent altogether (amenorrhea). As a result, women may require a number of tests to determine ovulatory status. Not all of these tests will be necessary in every case.
|
| |
| Serum FSH / LH Testing |
In some woman, blood tests to measure LH and FSH levels may be needed to check for hypothalamic pitutary dysfunction. This is a problem related to the release of LH and FSH from the pitutary gland. These tests are usually performed in the follicular phase of the menstrual cycle to detect hormonal abnormalities or defencies. |
| |
| Prolactin Testing |
Prolactin is the hormone that stimulates the production of breast milk in women. High levels of prolactin result in a condition known as hyperprolactinemia – a condition that interferes with ovulation. Blood tests to determine if this is the cause of an ovulatory problem are usually performed at the beginning of the cycle. |
| |
| Other Tests |
| |
 |
In certain cases , we may need to perform additional tests , including thyroid testing or serum progesterone, to further identify if there is a problem with ovulation. Structural problems, blockages and other disorders of the uterus, the fallopian tubes and the pelvis, may be diagnosed through a sophisticated x-ray study (or film) . A small tube is inserted into the cervix and a dye is injected slowly . The flow of the dye into the uterus, out through the fallopian tubes and into the pelvis can then be viewed on a screen . This test is performed after a menstrual period but before ovulation . During the injection of the dye , the woman may feel uterine cramping that may last several hours. |
After the test, there may be a sticky discharge for several hours as the dye is expelled from the uterus . A sanitory napkin is worn instead of a tampon to allow the fluid to escape. Whatever fluid remains in the pelvic cavity is absorbed by the body without harmful effects.
One positive potential effect of HSG testing is that the chance of conception appears to increase for several cycles after an oil dye is used . |
|
| |
| Diagnostic Laparoscopy |
| |
 |
Performed under general anaethesia , and usually in a hospital ,this test enables your doctor to directly view the outside of your uterus , the fallopian tubes , the ovaries and the pelvic cavity.An instrument is inserted through an incision in the abdomen . This procedure enables more detailed information to be obtained about these organs and detection of any adhesions that might be located around the fallopian tubes . It also helps to identify endometriosis , the presence of normal uterine tissue in abnormal places outside the uterus . Sometimes even minimal endometriosis can cause infertility.
Laproscopy is performed if endometriosis, tubal disorders or adhesions (scar tissue) are suspected , and it is genrally reserved for the end of the work-up. The incision is closed with several stitches that absorb within weeks. |
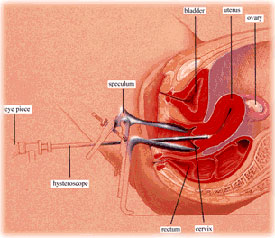
The procedure is scheduled before ovulation and is usually done as a 1-day surgery, enabling the woman to go home later that day. A sore throat, shoulder pain, a feeling of a bloated or swollen abdomen and general stiffness and soreness are commonly experienced for a day or two. Normal activities and work can soon be resumed. If it is felt necessary, a visual examination of the interior of the uterus to look for small growths(polyps, submucous fibroids), scars and / or abnormalities may also be be done at the time of the laproscopy. This is done by inserting a device directly into the uterus. The procedure adds only a few miniutes to the surgical time and does not cause any additional discomfort because the patient is already under anasthesia. |
|
|
Is there a problem with implantation ? |
|
| |
Infertility may be linked to problems in the development of the endometrium and the hormones that work to maintain pregnancy. These types pf problems are often referred to as luteal phase defects. Several tests can be used to identify a luteal phase defect. |
| |
| Serum Progesterone testing |
This blood testing is performed to determine the functioning of the corpus luteum, which produces the hormone progesterone. Progesterone controls the development of the lining of the uterus and prepares for the embryo implantation. If progesterone production is inadequate the endometrium will not be able to sustain the implantation of the embryo. Progesterone testing is usually performed about 7-9 days after suspected ovulation. |
| |
| Endometrial Biopsy |
In this test a tiny sample is removed from the endometrium ( uterine lining for microscopic study) This is done about 1-3 days before the beginning of menstruation as judged from BBT charts, urinary LH testing and usual menstrual history. The biopsy determines if proper development of the endometrium has occured so that fertilized egg can implant and be maintained. The biopsy is performed by passing a small instrument through the vagina into the uterus. The the collection of tissue takes only a moment, but may cause uterine cramps and slight discomfort for upto an hour. There may also be slight bleeding or spotting after the procedure. Although, the biopsy does not necessarily disturb an early pregnancy in the cycle of conception, patients should avoid conceiving in the month of the planned biopsy. Once the menstrual perid starts, the patient calls the clinic so that exact dating of the tissue can be recorded. It may take as long as 7-10 days to prepare and interpret the biopsy. |
| |
| Ultrasound Testing |
|
This painless test is performed 7-9 days after ovulation by applying a probe to the outside of the abdomen, or by inserting a diagnostic instrument into the vagina. High frequency sound waves produce pictures that reveal information about the development of the endometrium. The scan determines how thick the uterine lining is and how well the uterus is responding to hormone production. |
|
What is unexplained infertility? |
|
| |
If a factor causing the inability to conceive is not found after a complete evaluation, a couple is often said to have unexplained infertility. This occurs in about 10% to 15% of couples who seek help. Although the abilitiy to detect infertility problems is quite advanced the work-up may be unable to detect subtle or a yet unknown barriersto normal reproduction. |
|

 GETTING HELP FOR INFERTILITY TREATMENT
GETTING HELP FOR INFERTILITY TREATMENT

